For anti-racist dataviz, our most effective tool is context. The way that data is framed can make a very real impact on how it’s interpreted. For example, this case study from the New York Times shows two different framings of the same economic data and how, depending on where the author starts the X-Axis, it can tell 2 very different — but both accurate — stories about the subject.
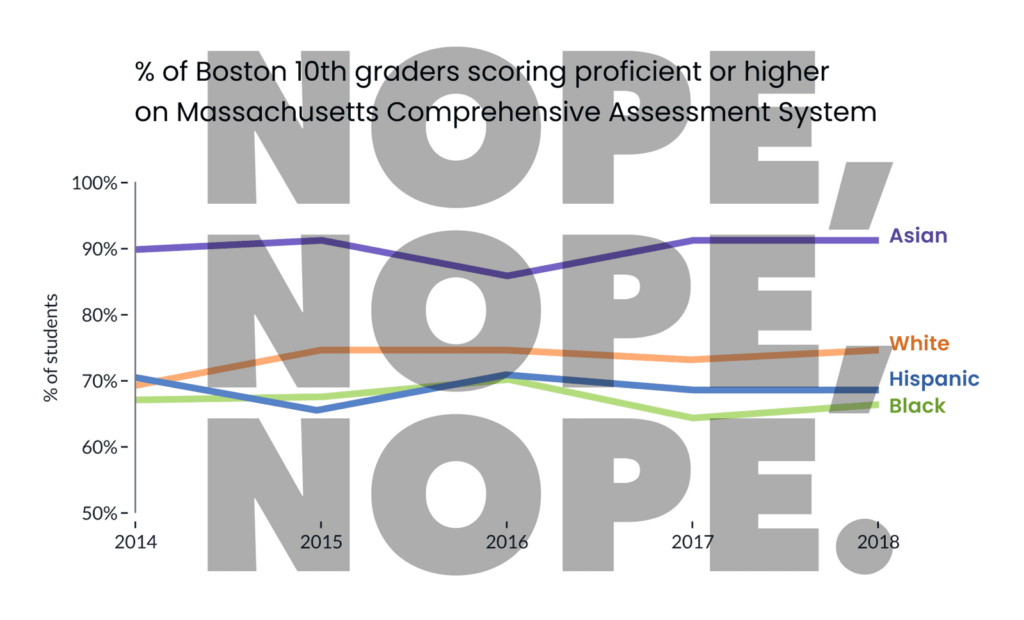
As Pieta previously highlighted, dataviz in spaces that address race / ethnicity are sensitive to “deficit framing.” That is, when it’s presented in a way that over-emphasizes differences between groups (while hiding the diversity of outcomes within groups), it promotes deficit thinking (see below) and can reinforce stereotypes about the (often minoritized) groups in focus.
In a follow up study, Eli and Cindy Xiong (of UMass’ HCI-VIS Lab) confirmed Pieta’s arguments, showing that even “neutral” data visualizations of outcome disparities can lead to deficit thinking (and therefore stereotyping) and that the way visualizations are designed can significantly impact these harmful tendencies.
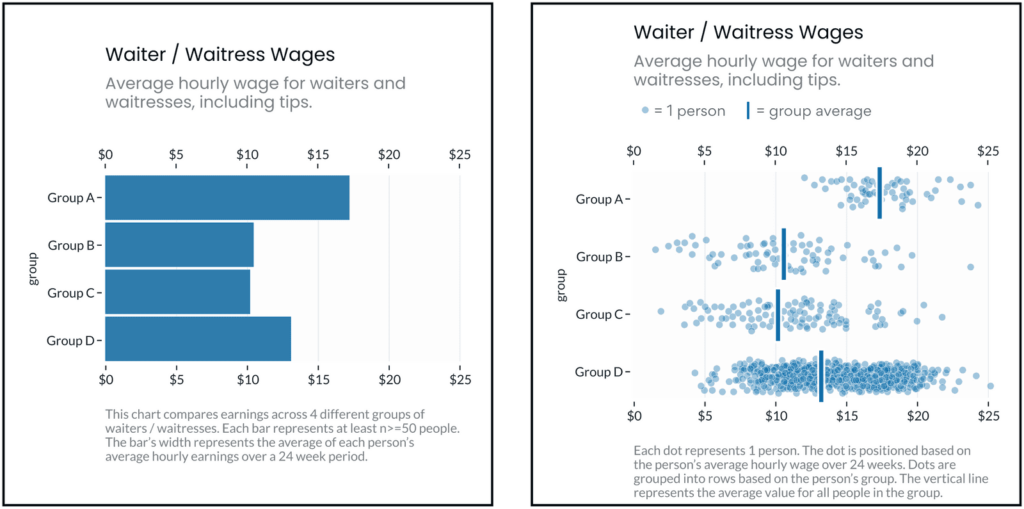
The same dataset, visualized two different ways. The left fixates on between-group differences, which can encourage stereotyping. The right shows both between and within group differences, which may discourage viewers’ tendencies to stereotype the groups being visualized.
Excerpt:
Ignoring or deemphasizing uncertainty in dataviz can create false impressions of group homogeneity (low outcome variance). If stereotypes stem from false impressions of group homogeneity, then the way visualizations represent uncertainty (or choose to ignore it) could exacerbate these false impressions of homogeneity and mislead viewers toward stereotyping.
If this is the case, then social-outcome-disparity visualizations that hide within-group variability (e.g. a bar chart without error bars) would elicit more harmful stereotyping than visualizations that emphasize within-group variance (e.g. a jitter plot).
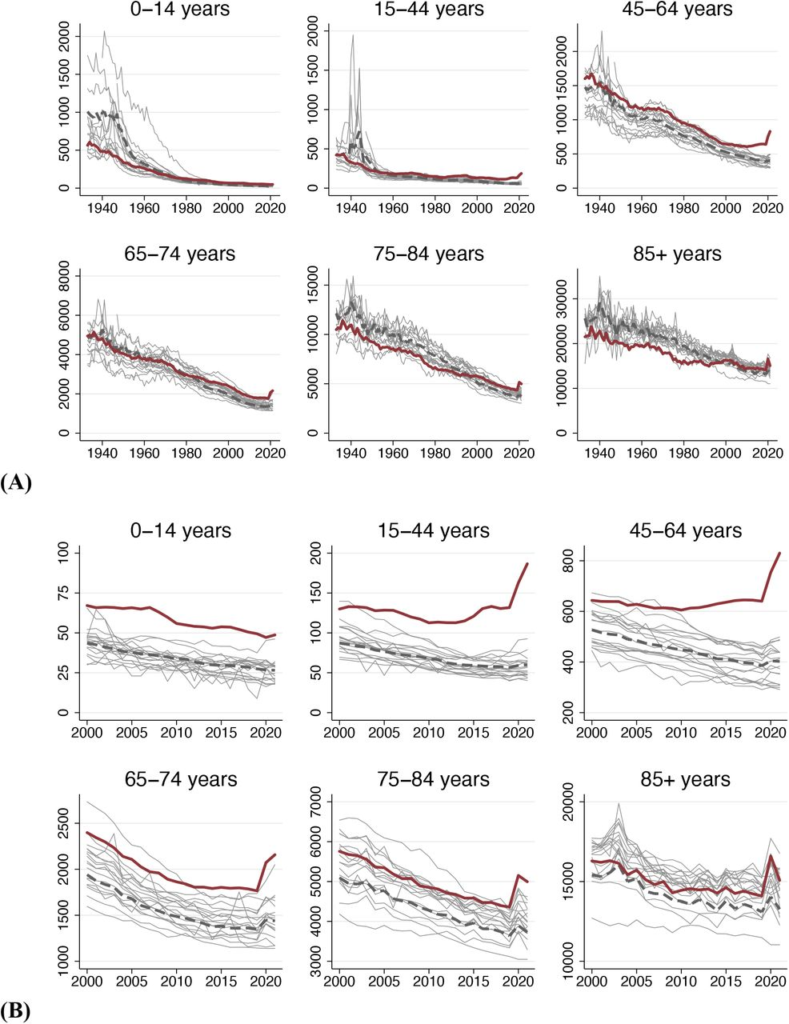
Age-specific mortality trends in the U.S. and other wealthy nations.Source: Human Mortality Database. Note: Figure shows deaths per 100K population, (A) 1933-2021 and (B) 2000-2021. Dark red line is U.S.; pink line is population-weighted average of other wealthy nations; grey lines are country-specific trends for other countries.
Excerpt:
We assessed how many U.S. deaths would have been averted each year, 1933-2021, if U.S. age-specific mortality rates had equaled those of other wealthy nations. The annual number of excess deaths in the U.S. increased steadily beginning in the late 1970s, reaching 626,353 in 2019. Excess deaths surged during the COVID-19 pandemic. In 2021, there were 1,092,293 “Missing Americans” and 25 million years of life lost due to excess mortality relative to peer nations. In 2021, half of all deaths under 65 years and 91% of the increase in under-65 mortality since 2019 would have been avoided if the U.S. had the mortality rates of its peers. Black and Native Americans made up a disproportionate share of Missing Americans, although the majority were White.
One sentence summary In 2021, 1.1 million U.S. deaths – including 1 in 2 deaths under age 65 years – would have been averted if the U.S. had the mortality rates of other wealthy nations.
Author(s):
Jacob Bor, View ORCID ProfileAndrew C. Stokes, Julia Raifman, Atheendar Venkataramani, Mary T. Bassett, David Himmelstein, Steffie Woolhandler
Over the past two decades, the U.S. maternal mortality rate has not improved while maternal mortality rates have decreased for other regions of the world. Furthermore, the rate at which women in the U.S. experience short-term or long-term negative health consequences due to unexpected outcomes of pregnancy or childbirth has also steadily increased over the past few decades, with nearly 50,000 women in the U.S. experiencing these health consequences in 2014. Significant racial and ethnic disparities persist in both the rate of women in the U.S. who die due to complications of pregnancy or delivery and the rate that women experience negative health consequences due to unexpected pregnancy or childbirth outcomes.
…..
Compared to any other racial or ethnic group,7 Black8 women experience the highest rates of nearly all of Centers for Disease Control and Prevention’s (CDC) severe maternal morbidity9 indicators.10 Black women in the U.S. are 3 to 4 times more likely to die from pregnancy-related complications than White11 women in the U.S., and Native American12 women are more than 2 times more likely to die from pregnancy-related complications than White women in the U.S.13 Pregnancy-related mortality is also slightly elevated for Asian women (a 1.1 disparity ratio),14 and for Hispanic women in some geographic areas.15 Moreover, the risk of pregnancy-related death is so elevated for Black women in certain regions of the U.S. that it is comparable to the
rate of pregnancy-related deaths16 in some developing countries.17 This racial disparity has not improved in decades,18 and is also seen in other middle to high-income countries with multiethnic populations.19 According to the World Health Organization (WHO), the U.S. maternal mortality ratio ranked 56th in the world in 2017.20 According to the National Center for Health Statistics (NCHS), in 2018, the maternal mortality rate in the U.S. was 17.4 maternal deaths per 100,000 live births, with 658 women dying of maternal causes.21 In 2019, the maternal mortality rate in the U.S. was 20.1 maternal deaths per 100,000 live births, with 754 women dying of maternal causes.
Heriot, Gail L., Dissenting Statement and Rebuttal of Commissioner Gail L. Heriot in U.S. Commission on Civil Right Report: Racial Disparities on Maternal Health (September 15, 2021). San Diego Legal Studies Paper 21-028, Available at SSRN: https://ssrn.com/abstract=3924645 or http://dx.doi.org/10.2139/ssrn.3924645
Abstract:
On September 15, 2021, the U.S. Commission on Civil Rights published a report entitled Racial Disparities in Maternal Health (the “Report”). This Dissenting Statement and Rebuttal (the “Statement”) is a part of that report.
Among other things, the Statement points out several errors in Report. For example, the Report incorrectly states that maternal mortality has increased 50% over the last generation. What has actually happened is that changes in death certificates have caused more deaths to be classified as maternal in nature. The Report also emphasizes the theory that racism plays a prominent role in causing racial disparities in maternal mortality. The Statement points out in response that maternal mortality rates for Hispanic and Asian American mothers are lower than the rate for white mothers. This tends to detract from the theory that racism is what’s causing the disparities.
Black pregnant women continue to face disproportionately high pregnancy-related deaths, with data from the Centers for Disease Control and Prevention indicating a 26 percent increase in the maternal mortality rate for Black women since the start of the pandemic.
Though researchers do not have an explanation for the disparities, the research suggests it’s a culmination of institutional racism and other health factors, such as the increased risk of obesity and hypertension in Black women. Howell also added that stress and a lack of access to quality prenatal care further exacerbates this issue.
“It really does boil down to how public health officials relate to Black women who are giving birth,” Howell said. “Statistics about Black maternal mortality are high across the board, no matter what your educational level is, no matter what your insurance level is.”
In 2018, tennis star Serena Williams opened up in an interview with Vogue magazine about encountering severe health complications after giving birth because doctors neglected to listen about her existing medical conditions.
“When you have someone like Serena Williams having problems giving birth, and not being treated properly by nurses and doctors when she complains about not feeling well, then you look at the doctor of someone who is poor in Louisiana, and has the same kind of problem — they are probably treated even worse,” Howell said.
Arlington, VA – Two newresearch reports designed to guide the insurance industry toward proactive, quantitative solutions to identify, measure and address potential racial bias in insurance pricing were published by the Casualty Actuarial Society (CAS) today.
“These two new reports in our CAS Research Series on Race and Insurance Pricing continue to provide additional insight into industry discussions on this topic,” said Victor Carter-Bey, DM, CAS chief executive officer. “We hope with this series to serve as a thought leader and role model for other insurance organizations and corporations in promoting fairness and progress.”
As the professional society of actuaries specializing in property and casualty insurance, the CAS is committed to diversity, equity and inclusion in actuarial work. To this end, the Society is releasing a series of four CAS Research Papers, which support the CAS’s Approach to Race and Insurance Pricing. This approach was adopted by the CAS Board of Directors in December 2020 and includes four key areas of focus and goals: basic and continuing education, research, leadership and influence, and collaboration. Each paper in the series addresses a different aspect of race and insurance pricing as viewed through the lens of property and casualty insurance.
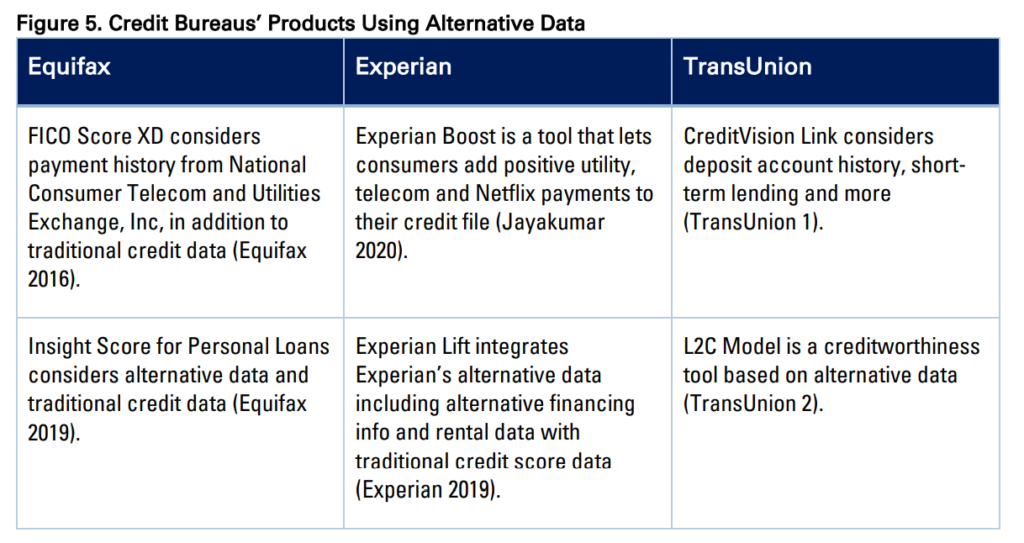
Defining Discrimination in Insurance. This report examines terms that are being used in discussions around potential discrimination in insurance, including protected class, unfair discrimination, proxy discrimination, disparate impact, disparate treatment, and disproportionate impact. The paper provides historical and practical context for these terms and illustrates the inconsistencies in how different stakeholders define them. It also describes the potential impacts of these definitions on actuarial work.
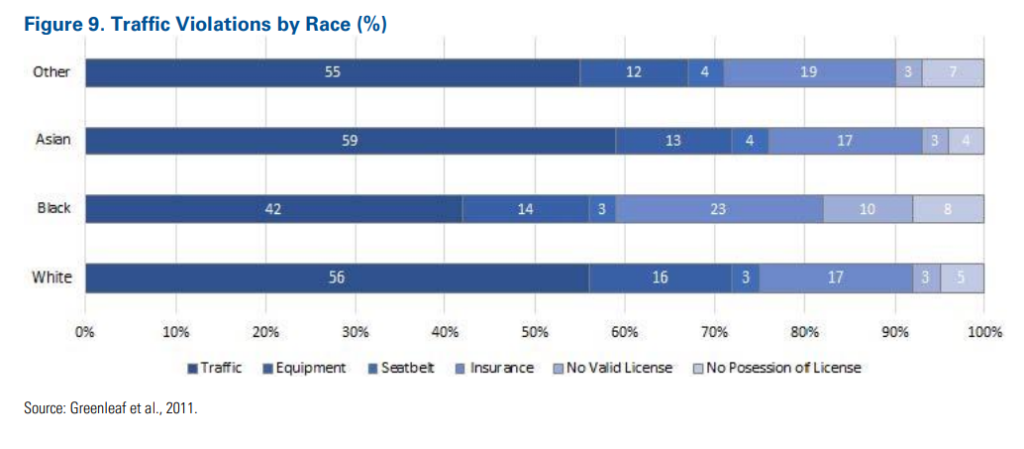
Understanding Potential Influences of Racial Bias on P&C Insurance: Four Rating Factors Explored. The paper examines four commonly used rating factors to understand how the data underlying insurance pricing models may be impacted by racially biased policies and practices outside of insurance. The goal is to highlight the multi-dimensional impacts of systemic racial bias, as it may relate to insurance pricing. The four factors included in the report are: Credit-Based Insurance Score (CBIS), geographic location, homeownership and Motor Vehicle Records.
These four research reports are just one way the CAS supports evolving actuarial practices and strengthens the knowledge of its members. The papers demonstrate the Society’s recognition that actuaries—who are responsible for setting insurance rates—must be a voice in an ever-evolving dialogue. The CAS understands that this work is critical to maintaining the Society and its members’ public trust.
The goal of this paper is to equip actuaries to proactively participate in discussions and actions related to potential racial biases in insurance practices. This paper uses the following definition of racial bias: Racial bias refers to a system that is inherently skewed along racial lines. Racial bias can be intentional or unintentional and can be present in the inputs, design, implementation, interpretation or outcomes of any system. To support actuaries and the insurance industry in these efforts, this paper examines issues of racial bias that have impacted four areas of noninsurance financial services — mortgage lending, personal lending, commercial lending and the underlying credit-scoring systems — as well as the solutions that have been implemented in these sectors to address this bias. Actuaries are encouraged to combine this information on solutions and gaps in other industries with expertise in their practice areas to determine how, if at all, this information could be applied to identify potential racial biases impacting insurance or other industries in which actuaries work. Parallels can be drawn between the issues noted here in financial services and those being discussed within the insurance industry. While many states have long considered race to be a protected class which cannot be used for insurance business decisions, regulators and consumer groups have brought forth concerns about potential racial bias implicit in existing practices or apparent in insurance outcomes. State regulators are taking individual actions to address potential issues through prohibition of certain rating factors, and even some insurers are proactively calling for the industry to move away from using information thought to be correlated with race. However, this research suggests that government prohibition of specific practices may not be a silver-bullet solution. Actuaries can play a key role as the insurance industry develops approaches to test for, measure and address potential racial bias, and increase fairness and equality in insurance, while still maintaining riskbased pricing, company competitiveness and solvency.
Author(s): Members of the 2021 CAS Race and Insurance Research Task Force
Insurance rating characteristics have come under scrutiny by legislators and regulators in their efforts to identify and address racial bias in insurance practices. The goal of this paper is to equip actuaries with the information needed to proactively participate in industry discussions and actions related to racial bias and insurance rating factors. This paper uses the following definition of racial bias: Racial bias refers to a system that is inherently skewed along racial lines. Racial bias can be intentional or unintentional and can be present in the inputs, design, implementation, interpretation, or outcomes of any system. This paper will examine four commonly used rating factors in personal lines insurance — credit-based insurance score, geographic location, home ownership, and motor vehicle records — to understand how the data underlying insurance pricing models may be impacted by racially biased policies and practices outside of the system of insurance. Historical issues like redlining and racial segregation, as well as inconsistent enforcement of policies and practices contribute to this potential bias. These historical issues do not necessarily change the validity of the actuarial approach of evaluating statistical correlation of rating factors to insurance loss overall. Differences in the way individual insurers build rating models may produce very different end results for customers. More data and analyses are needed to understand if and to what extent these specific issues of racial bias impact insurance outcomes. Actuaries and other readers can combine this information with their own subject matter expertise to determine if and how this could impact the systems for which they are responsible, and what actions, if any, could be taken as a result.
Author(s): Members of the 2021 CAS Race and Insurance Research Task Force
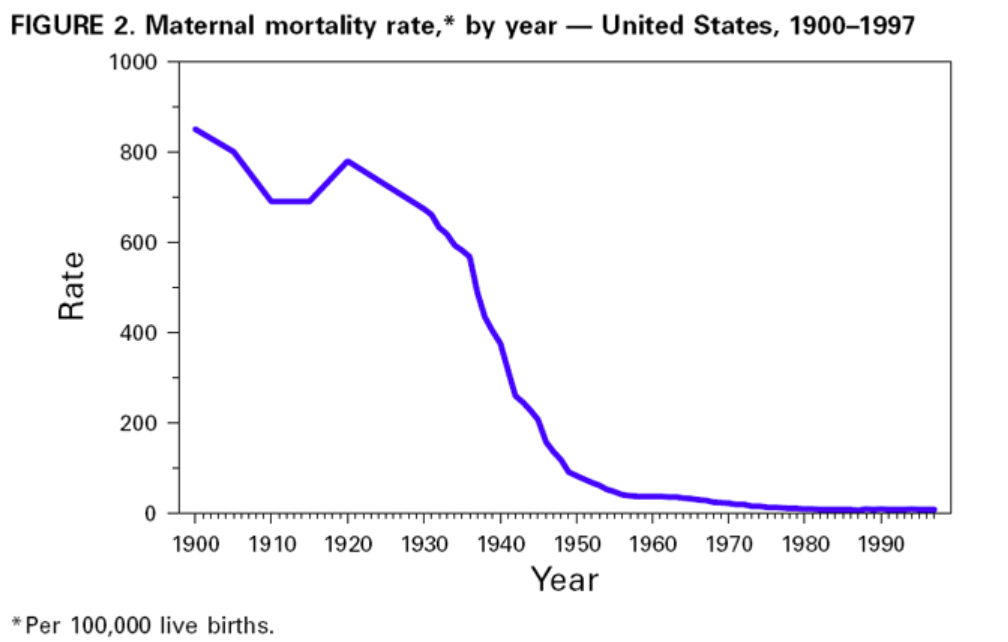
Despite the dramatic decline in infant and maternal mortality during the 20th century, challenges remain. Perhaps the greatest is the persistent difference in maternal and infant health among various racial/ethnic groups, particularly between black and white women and infants. Although overall rates have plummeted, black infants are more than twice as likely to die as white infants; this ratio has increased in recent decades. The higher risk for infant mortality among blacks compared with whites is attributed to higher LBW incidence and preterm births and to a higher risk for death among normal birthweight infants (greater than or equal to 5 lbs, 8 oz [greater than or equal to 2500 g]) (18). American Indian/ Alaska Native infants have higher death rates than white infants because of higher SIDS rates. Hispanics of Puerto Rican origin have higher death rates than white infants because of higher LBW rates (19). The gap in maternal mortality between black and white women has increased since the early 1900s. During the first decades of the 20th century, black women were twice as likely to die of pregnancy-related complications as white women. Today, black women are more than three times as likely to die as white women.
During the last few decades, the key reason for the decline in neonatal mortality has been the improved rates of survival among LBW babies, not the reduction in the incidence of LBW. The long-term effects of LBW include neurologic disorders, learning disabilities, and delayed development (20). During the 1990s, the increased use of assisted reproductive technology has led to an increase in multiple gestations and a concomitant increase in the preterm delivery and LBW rates (21). Therefore, in the coming decades, public health programs will need to address the two leading causes of infant mortality: deaths related to LBW and preterm births and congenital anomalies. Additional substantial decline in neonatal mortality will require effective strategies to reduce LBW and preterm births. This will be especially important in reducing racial/ethnic disparities in the health of infants.
Approximately half of all pregnancies in the United States are unintended, including approximately three quarters among women aged less than 20 years. Unintended pregnancy is associated with increased morbidity and mortality for the mother and infant. Lifestyle factors (e.g., smoking, drinking alcohol, unsafe sex practices, and poor nutrition) and inadequate intake of foods containing folic acid pose serious health hazards to the mother and fetus and are more common among women with unintended pregnancies. In addition, one fifth of all pregnant women and approximately half of women with unintended pregnancies do not start prenatal care during the first trimester. Effective strategies to reduce unintended pregnancy, to eliminate exposure to unhealthy lifestyle factors, and to ensure that all women begin prenatal care early are important challenges for the next century.
Author(s): Division of Reproductive Health, National Center for Chronic Disease Prevention and Health Promotion, CDC.
The research showed that the rate at which older workers left employment increased dramatically during the pandemic.
This was especially the case with women — an 8-percentage-point increase vs. 7 points for men; Asian Americans — a 13-point increase; those with less than a college degree — a 10-point increase; and workers with occupations that did not lend themselves to remote work.
….
There was one exception: Workers 70 and older were 5.9 percentage points more likely to leave the workforce and retire. The study noted that these workers were likely already receiving Social Security benefits, so claiming did not markedly increase.
Among all workers 55 and older, the monthly claiming rate for Social Security benefits remained constant between April 2019 and June 2021, the researchers found.
The use of the CKD-EPI 2021 eGFR creatinine equation for calculating eGFRcr in adults.2,3 This new equation is recommended because a race coefficient is not included in its computation and reporting. The CKD-EPI 2021 eGFR creatinine equation included diversity in its development and does not disproportionately affect any one group.3
National efforts are also underway to facilitate increased, routine, and timely use of cystatin C (CPT 82610), especially to further evaluate eGFRcr in adults who are at risk for or have chronic kidney disease, or in individuals with abnormally high or low muscle mass. The CKD-EPI 2021 eGFR using creatinine and cystatin C (eGFRcr-cys) is more accurate, more closely approximates measured GFR and supports better clinical decisions than either marker alone.2,3