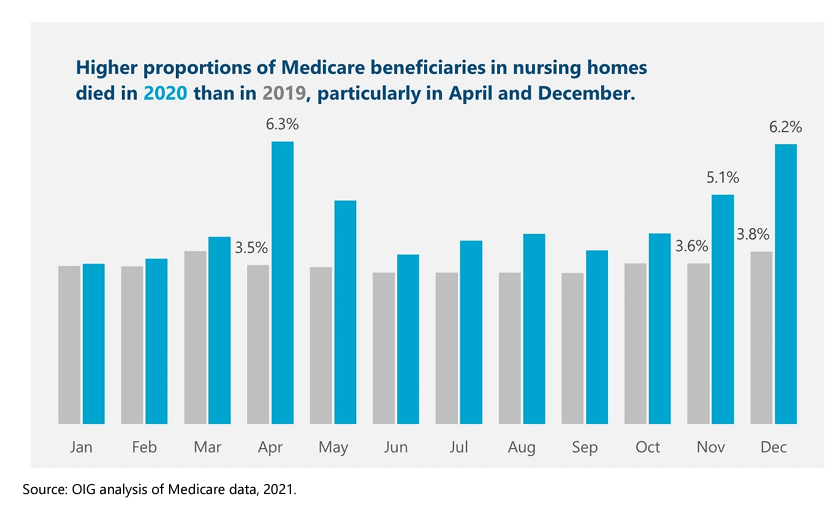
The overall mortality rate in nursing homes rose 32 percent in 2020. The pandemic had far-reaching implications for all nursing home beneficiaries, beyond those who had or likely had COVID-19. Among all Medicare beneficiaries in nursing homes, 22.5 percent died in 2020, which is an increase of one-third from 2019 when 17.0 percent of Medicare beneficiaries in nursing homes died. This 32-percent increase amounts to 169,291 more deaths in 2020 than if the mortality rate had remained the same as in 2019. Each month of 2020 had a higher mortality rate than the corresponding month a year earlier.
Almost 1,000 more beneficiaries died per day in April 2020 than in the previous year. In April 2020 alone, a total of 81,484 Medicare beneficiaries in nursing homes died. This is almost 30,000 more deaths—an average of about 1,000 per day—compared to the previous year. This increase in number occurred even though the nursing home population was smaller in April 2020. Overall, Medicare beneficiaries in nursing homes were almost twice as likely to die in April 2020 than in April 2019. In April 2020, 6.3 percent of all Medicare beneficiaries in nursing homes died, whereas 3.5 percent died in April 2019.
The mortality rates also rose at the end of 2020. In November, 5.1 percent of all Medicare beneficiaries in nursing homes died, and in December that increased to 6.2 percent. Again, these rates are markedly higher than the previous year. In November 2019, 3.6 percent of all Medicare beneficiaries in nursing homes died, and, in December 2019, 3.8 percent did.
Author(s): Jenell Clarke-Whyte and team
Publication Date: June 2021
Publication Site: Office of Inspector General, HHS
With the recent discovery that the CDC drafted — but never sent — a Health Alert in May 2021 about myocarditis after mRNA vaccination, I put together this timeline about vaccine myocarditis news and updates from government officials. I include a combination of documents from CDC and FDA, as well as what was covered in the mainstream media.
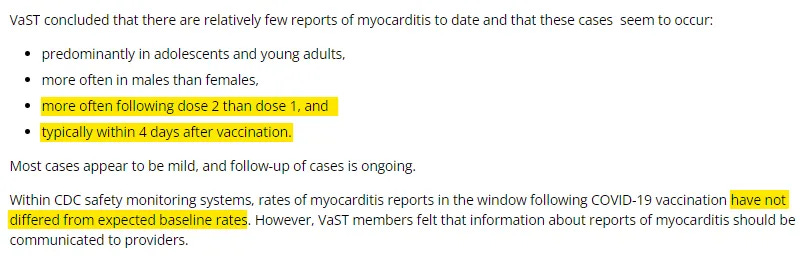
I think this timeline shows a pattern in which CDC & FDA failed to adequately investigate and inform the public about the risks of myocarditis early in the vaccine rollout. However, there was public acknowledgement by the CDC, as early as May 20, 2021, about a potential pattern of myocarditis after the 2nd dose of mRNA vaccines, particularly in young men.
On June 1, 2021, the CDC confirmed that they had identified a higher than expected signal of myocarditis for young men after mRNA vaccination, but that they still recommended Covid vaccination for everyone in this age group. Despite a lot more analysis and discussion of myocarditis after that, and a changing landscape with widespread natural immunity, the CDC & FDA position has changed very little since that time.
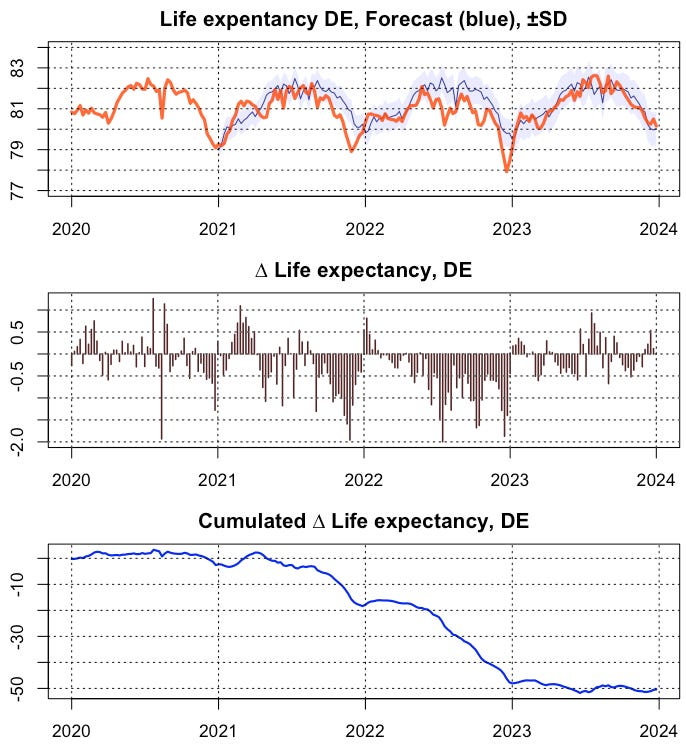
Destatis yesterday published deaths figures for the whole of 2023. In order to obtain a reliable assessment of the situation, I calculated the weekly time series of life expectancy, applied an ARIMA forecast from the reference epoch 2016-2020 and compared it with the actual values. In this way, results are now available for all 4 pandemic years to date (Fig. 1)
More than two dozen attorneys general are urging Food and Drug Administration officials to take urgent action to address disparities in how well pulse oximeters, the fingertip devices used to monitor a person’s oxygen levels, work on people with darker skin.
In a Nov. 1 letter, the AGs noted that it had been a year since the FDA convened a public meeting of experts, who called for clearer labeling and more rigorous testing of the devices, and that no action had been taken.
“We, the undersigned Attorneys General, write to encourage the FDA to act with urgency to address the inaccuracy of pulse oximetry when used on people with darker toned skin,” said the letter, written by California Attorney General Rob Bonta and signed by 24 other attorneys general.
Pulse oximeters’ overestimation of oxygen levels in patients with darker skin has, in a slew of recent research studies, been linked to poorer outcomes for many patients because of delayed diagnosis, delayed hospital admissions, and delayed access to treatment, including for severe Covid-19 infections. Higher amounts of pigments called melanin in darker skin interfere with the ability of light-based sensors in pulse oximeters to detect oxygen levels in blood.
….
The delay has frustrated health care workers who use pulse oximeters and have studied them and followed the progress toward creating new devices that work better. “I just get mad that these things are not on the market,” Theodore J. Iwashyna, an ICU physician at Johns Hopkins, told STAT. “Just last week in my ICU, I had a patient whose pulse oximeter was reading 100% at the same time that his arterial blood gas showed that his oxygen levels were dangerously low. I need these things to work, and work in all my patients.”
For decades, runaway Medicare spending was the story of the federal budget.
Now, flat Medicare spending might be a bigger one.
Something strange has been happening in this giant federal program. Instead of growing and growing, as it always had before, spending per Medicare beneficiary has nearly leveled off over more than a decade.
The trend can be a little hard to see because, as baby boomers have aged, the number of people using Medicare has grown. But it has had enormous consequences for federal spending. Budget news often sounds apocalyptic, but the Medicare trend has been unexpectedly good for federal spending, saving taxpayers a huge amount relative to projections.
….
Some of the reductions are easy to explain. Congress changed Medicare policy. The biggest such shift came with the Affordable Care Act in 2010, which reduced Medicare‘s payments to hospitals and to health insurers that offered private Medicare Advantage plans. Congress also cut Medicare payments as part of a budget deal in 2011.
But most of the savings can’t be attributed to any obvious policy shift. In a recent letter to the Senate Budget Committee, economists at the Congressional Budget Office described the huge reductions in its Medicare forecasts between 2010 and 2020. Most of those reductions came from a category the budget office calls “technical adjustments,” which it uses to describe changes to public health and the practice of medicine itself.
Older Americans appear to be having fewer heart attacks and strokes, the likely result of effective cholesterol and blood pressure medicines that became cheap and widely used in recent years, according to research from Professor Cutler and colleagues. And drug makers and surgeons haven’t developed as many new blockbuster treatments recently — there has been no new Prozac or angioplasty to drive up spending. (Medicare is currently barred by statute from covering the new class of expensive anti-obesity drugs.)
….
Medicare may even wind up saving money because of Covid-19 — because the older Americans who died from the disease tended to have other illnesses that would have been expensive to treat if they had survived, according to an analysis from the Medicare actuary.
Question Was political party affiliation a risk factor associated with excess mortality during the COVID-19 pandemic in Florida and Ohio?
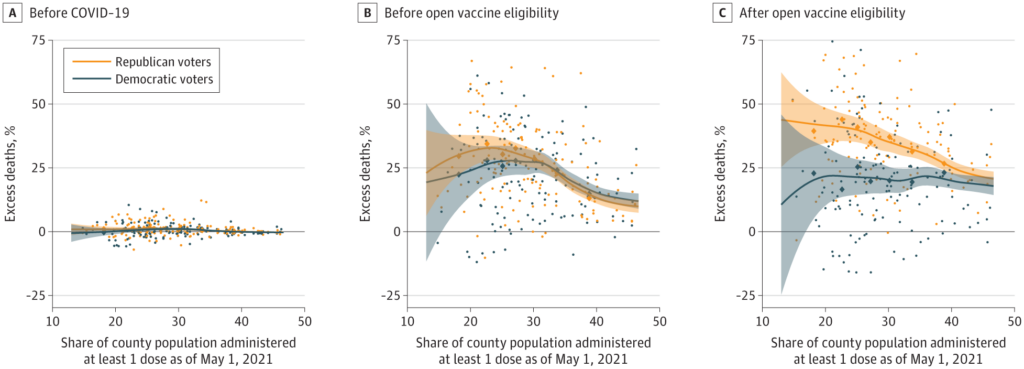
Findings In this cohort study evaluating 538 159 deaths in individuals aged 25 years and older in Florida and Ohio between March 2020 and December 2021, excess mortality was significantly higher for Republican voters than Democratic voters after COVID-19 vaccines were available to all adults, but not before. These differences were concentrated in counties with lower vaccination rates, and primarily noted in voters residing in Ohio.
Meaning The differences in excess mortality by political party affiliation after COVID-19 vaccines were available to all adults suggest that differences in vaccination attitudes and reported uptake between Republican and Democratic voters may have been a factor in the severity and trajectory of the pandemic in the US.
Abstract
Importance There is evidence that Republican-leaning counties have had higher COVID-19 death rates than Democratic-leaning counties and similar evidence of an association between political party affiliation and attitudes regarding COVID-19 vaccination; further data on these rates may be useful.
Objective To assess political party affiliation and mortality rates for individuals during the initial 22 months of the COVID-19 pandemic.
Design, Setting, and Participants A cross-sectional comparison of excess mortality between registered Republican and Democratic voters between March 2020 and December 2021 adjusted for age and state of voter registration was conducted. Voter and mortality data from Florida and Ohio in 2017 linked to mortality records for January 1, 2018, to December 31, 2021, were used in data analysis.
Exposures Political party affiliation.
Main Outcomes and Measures Excess weekly deaths during the COVID-19 pandemic adjusted for age, county, party affiliation, and seasonality.
Results Between January 1, 2018, and December 31, 2021, there were 538 159 individuals in Ohio and Florida who died at age 25 years or older in the study sample. The median age at death was 78 years (IQR, 71-89 years). Overall, the excess death rate for Republican voters was 2.8 percentage points, or 15%, higher than the excess death rate for Democratic voters (95% prediction interval [PI], 1.6-3.7 percentage points). After May 1, 2021, when vaccines were available to all adults, the excess death rate gap between Republican and Democratic voters widened from −0.9 percentage point (95% PI, −2.5 to 0.3 percentage points) to 7.7 percentage points (95% PI, 6.0-9.3 percentage points) in the adjusted analysis; the excess death rate among Republican voters was 43% higher than the excess death rate among Democratic voters. The gap in excess death rates between Republican and Democratic voters was larger in counties with lower vaccination rates and was primarily noted in voters residing in Ohio.
Conclusions and Relevance In this cross-sectional study, an association was observed between political party affiliation and excess deaths in Ohio and Florida after COVID-19 vaccines were available to all adults. These findings suggest that differences in vaccination attitudes and reported uptake between Republican and Democratic voters may have been factors in the severity and trajectory of the pandemic in the US.
Author(s): Jacob Wallace, PhD1; Paul Goldsmith-Pinkham, PhD2; Jason L. Schwartz, PhD1
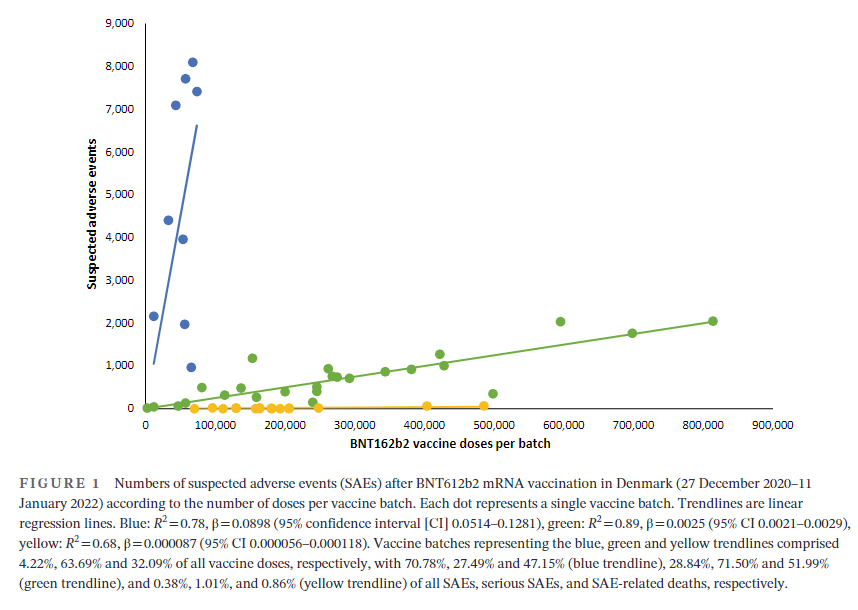
Vaccination has been widely implemented for mitigation of coronavirus disease-2019 (Covid-19), and by 11 November 2022, 701 million doses of the BNT162b2 mRNA vaccine (Pfizer-BioNTech) had been administered and linked with 971,021 reports of suspected adverse effects (SAEs) in the European Union/European Economic Area (EU/EEA).1 Vaccine vials with individual doses are supplied in batches with stringent quality control to ensure batch and dose uniformity.2 Clinical data on individual vaccine batch levels have not been reported and batch-dependent variation in the clinical efficacy and safety of authorized vaccines would appear to be highly unlikely. However, not least in view of the emergency use market authorization and rapid implementation of large-scale vaccination programs, the possibility of batch-dependent variation appears worthy of investigation. We therefore examined rates of SAEs between different BNT162b2 vaccine batches administered in Denmark (population 5.8 million) from 27 December 2020 to 11 January 2022.
….
A total of 7,835,280 doses were administered to 3,748,215 persons with the use of 52 different BNT162b2 vaccine batches (2340–814,320 doses per batch) and 43,496 SAEs were registered in 13,635 persons, equaling 3.19 ± 0.03 (mean ± SEM) SAEs per person. In each person, individual SAEs were associated with vaccine doses from 1.531 ± 0.004 batches resulting in a total of 66,587 SAEs distributed between the 52 batches. Batch labels were incompletely registered or missing for 7.11% of SAEs, leaving 61,847 batch-identifiable SAEs for further analysis of which 14,509 (23.5%) were classified as severe SAEs and 579 (0.9%) were SAE-related deaths. Unexpectedly, rates of SAEs per 1000 doses varied considerably between vaccine batches with 2.32 (0.09–3.59) (median [interquartile range]) SAEs per 1000 doses, and significant heterogeneity (p < .0001) was observed in the relationship between numbers of SAEs per 1000 doses and numbers of doses in the individual batches. Three predominant trendlines were discerned, with noticeable lower SAE rates in larger vaccine batches and additional batch-dependent heterogeneity in the distribution of SAE seriousness between the batches representing the three trendlines (Figure 1). Compared to the rates of all SAEs, serious SAEs and SAE-related deaths per 1.000 doses were much less frequent and numbers of these SAEs per 1000 doses displayed considerably greater variability between batches, with lesser separation between the three trendlines (not shown).
Author(s): Max Schmeling, Vibeke Manniche, Peter Riis Hansen
Publication Date: 30 Mar 2023
Publication Site: European Journal of Clinical Investigation
One thing that is tied to the national emergency is an extension of COBRA deadlines for people who are out of work. These deadlines are extended during the “outbreak period” which ends 60 days after the end of the national emergency.
The DHS rules for vaccine mandates for foreign travelers at land border crossings from Canada and Mexico rely on the national emergency as their legal basis, so theoretically they will end with the national emergency. But there has been no official actions to lift those rules, and I suspect the White House expects this vaccine mandate to continue for at least another month. (See section on travel vaccine mandates further down for more details.)
JAMA Health Forum. 2023;4(3):e230010. doi:10.1001/jamahealthforum.2023.0010
Graphic:
Excerpt:
Key Points
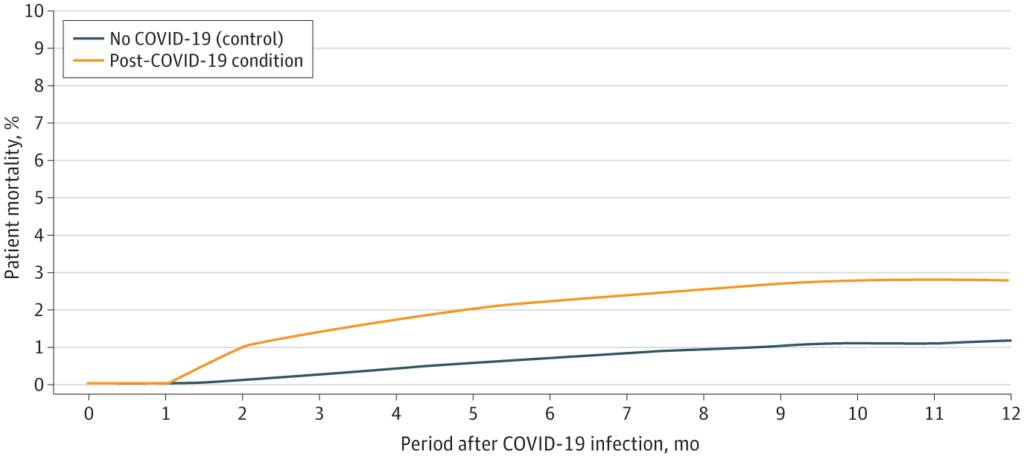
Question Do postacute sequelae of SARS-CoV-2 increase risks of 1-year adverse outcomes?
Findings In this case-control study of 13 435 US adults with post–COVID-19 condition (PCC) and 26 870 matched adults without COVID-19, the adults with PCC experienced increased risks for a number of cardiovascular outcomes, such as ischemic stroke. During the 12-month follow-up period, 2.8% of the individuals with PCC vs 1.2% of the individuals without COVID-19 died, implying an excess death rate of 16.4 per 1000 individuals.
Meaning Individuals with PCC may be at increased risk for adverse outcomes in the year following initial infection.
Author(s): Andrea DeVries, PhD1; Sonali Shambhu, BDS, MPH1; Sue Sloop, PhD1; et al
A giant health insurer says health plan enrollees who suffered from long COVID-19 symptoms were more than twice as likely as other enrollees to die during a 12-month follow-up period.
Andrea DeVries, a researcher at Elevance Health, and three colleagues found that, during the year studied, 2.8% of the 13,435 enrollees classified as having “post-COVID-19 condition” died, according to a study published in the JAMA Health Forum, which is affiliated with the Journal of the American Medical Association.
That compares with a death rate of just 1.2% for similar enrollees without COVID-19 during the same period.
….
Elevance Health is the company formerly known as Anthem. The company provides or administers major medical coverage for about 48 million people.
The DeVries looked at claim records for 249,013 Elevance plan enrollees ages and older who were diagnosed with COVID-19 from April 1, 2020, through July 31, 2020 — before regulators had adopted a long COVID diagnosis code.
The team began by identifying enrollees with COVID-19 who had been enrolled in an Elevance plan for at least five months before being diagnosed with COVID-19 and who had survived for at least two months after the diagnosis date.
Because of the lack of a long COVID-19 diagnosis code, the team used claims for other conditions, such as loss of the sense of smell, brain fog, anxiety and heart rate problems, to come up with a list of enrollees with long COVID.
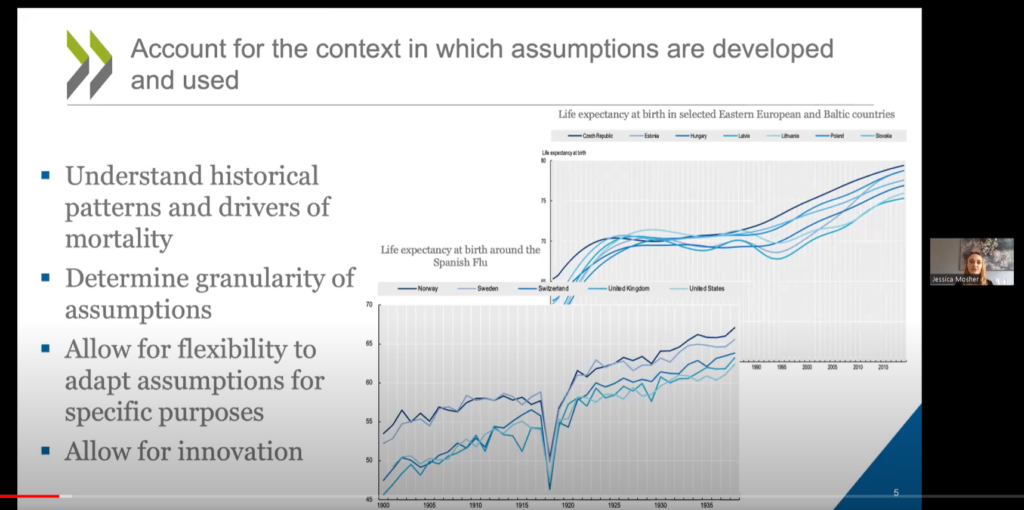
The report analyses the development of mortality assumptions to build mortality tables to better protect retirement income provision. It first provides an international overview of longevity trends and drivers over the last several decades, including the impact of the COVID-19 pandemic. It then explores considerations and traditional approaches for developing mortality tables, and details the standard mortality tables developed across OECD member countries. It concludes with guidelines to assist regulators and supervisors in assessing whether the mortality assumptions and tables used in the context of retirement income provision are appropriate.
The OECD will provide an overview of the publication, followed by a roundtable discussion with government and industry stakeholders. Topics discussed will include:
Recent mortality trends and drivers
How mortality trends/drivers can inform future expectations, and how to account for that in modelling
The challenge of accounting for COVID in setting mortality assumptions
Trade-offs for different modelling approaches
The usefulness of the guidelines included in the report in practice
How to better communicate around mortality assumptions to non-experts
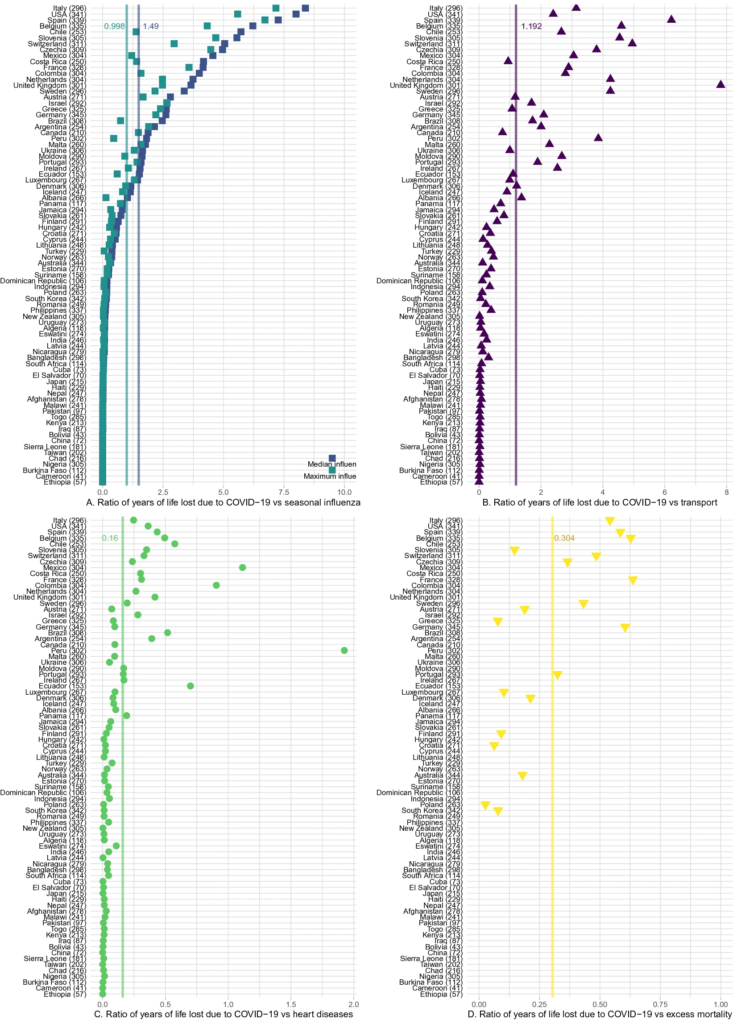
Understanding the mortality impact of COVID-19 requires not only counting the dead, but analyzing how premature the deaths are. We calculate years of life lost (YLL) across 81 countries due to COVID-19 attributable deaths, and also conduct an analysis based on estimated excess deaths. We find that over 20.5 million years of life have been lost to COVID-19 globally. As of January 6, 2021, YLL in heavily affected countries are 2–9 times the average seasonal influenza; three quarters of the YLL result from deaths in ages below 75 and almost a third from deaths below 55; and men have lost 45% more life years than women. The results confirm the large mortality impact of COVID-19 among the elderly. They also call for heightened awareness in devising policies that protect vulnerable demographics losing the largest number of life-years.
Author(s): Héctor Pifarré i Arolas, Enrique Acosta, Guillem López-Casasnovas, Adeline Lo, Catia Nicodemo, Tim Riffe & Mikko Myrskylä