Since the COVID-19 pandemic began, in early 2020, Globe Life has been one of the life insurers that’s been quickest to give analysts candid assessments of U.S. mortality.
Mortality is much lower than it was when pandemic-related mortality was peaking, and mortality trends are now helping, not, hurting, Globe Life’s earnings, Kalmbach said.
“Mortality has been fairly consistent over the last few quarters, which has been good,” he said.
He sees the mortality rate from accidents and other nonmedical causes improving.
….
“Heart disease and cancer, although improved, are still a little bit higher,” he said. “Another one that remains elevated as a cause of death is neurological disorders, which would be stroke and Alzheimer’s. We’re keeping an eye on that.”
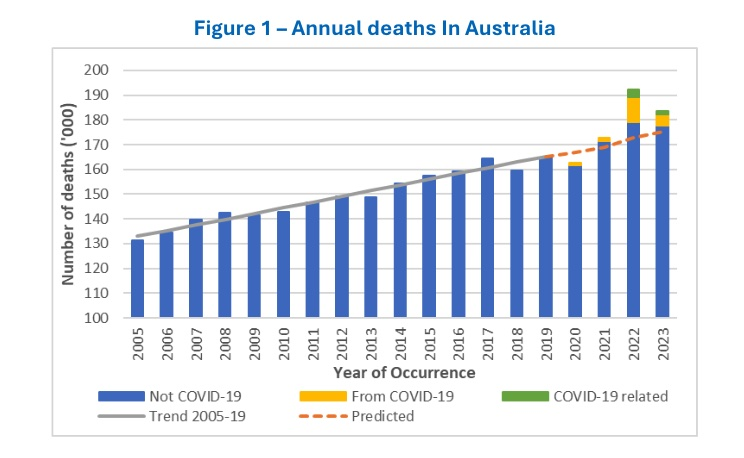
There were 8,400 more deaths in Australia in 2023 than predicted had the pandemic not occurred – less than half of the almost 20,000 excess deaths estimated for 2022.
The new Research Paper from the Mortality Working Group explores how COVID-19 affected mortality in Australia from 2020 to 2023 and how Australia’s experience compares with the rest of the world.
In brief:
The steep decline in excess deaths in 2023 was primarily due to the number of people dying from COVID-19 falling to 4,600 in 2023 from 10,300 in 2022.
While Australia’s excess mortality rate had dropped substantially, it remains significantly higher than the 1-2% excess observed in years of high flu deaths prior to the pandemic.
When analysing the excess mortality of 40 countries from 2020 to 2023, Australia’s excess mortality over the four-year period (5%) was low by global standards (11%).
Author(s): Mortality Working Group. Members Karen Cutter, Ronald Lai, Jennifer Lang, Han Li, Richard Lyon, Matt Ralph, Amitoze Singh, Michael Seymour, Zhan Wang.
Are we all really living longer? Let’s first point out that Princeton economists Anne Case and Angus Deaton, noted for their research in health and economics, recently showed that many Americans are not, in fact, enjoying extended lives. As they stated in their own New York Times op-ed, those without college degrees are “scarred by death and a staggeringly shorter life span.” According to their investigation, the expected lifespan for this group has been falling since 2010. By 2021, people without college degrees were expected to live to about 75, nearly 8.5 years shorter than their college-educated counterparts.
Overall life expectancy in America dropped in 2020 and 2021, with increases in mortality across the leading causes of death and among all ages, not just due to COVID-19. In August 2022, data confirmed that Americans are dying younger across all demographics. Again, the U.S. is an outlier. It was one of two developed countries where life expectancy did not bounce back in the second year of the pandemic.
So the argument that everyone is living longer greatly stretches the truth—unless, of course, you happen to be rich: A Harvard study revealed that the wealthiest Americans enjoy a life expectancy over a decade longer than their poorest counterparts.
Could the idea that working into our seventies and beyond boosts our health and well-being hold true? Obviously, for those in physically demanding roles, such as construction or mining, prolonged work is likely to lead to a higher risk of injury, accidents, and wearing down health-wise. But what about everybody else? What if you have a desk job? Wouldn’t it be great to get out there, do something meaningful, and interact with people, too?
Perhaps it’s easy for people like Steuerle and Kramon to imagine older people working in secure, dignified positions that might offer health benefits into old age – after all, those are the types of positions they know best.
But the reality is different. Economist Teresa Ghilarducci, a professor at the New School for Social Research, focuses on the economic security of older workers and flaws in U.S. retirement systems in her new book, Work, Retire, Repeat: The Uncertainty of Retirement in the New Economy. She calls those praising the health perks of working longer “oddballs” – those fortunate folks in cushy positions who have a lot of autonomy and purpose. Like lawmakers or tenured professors, for example.
Author(s): Lynn Parramore
Publication Date: 8 May 2024
Publication Site: Institute for New Economic Thinking
Chris Swift, the chief executive officer of Hartford Financial, on Friday confirmed what government statistics seem to be showing: The U.S. death rate continues to be noticeably higher than it was before early 2020, when the COVID-19 pandemic came to light.
Swift talked about the effects of the higher U.S. mortality rate on the company’s group life insurance business Friday during a conference call with securities analysts.
He noted that mortality was much lower in the first quarter than in the first quarter of 2023, but that it was still somewhat higher than the pre-pandemic average.
“The trends are downward,” Swift said. “But we believe that we’re still operating in an endemic state of mortality, which means it’s going to be higher than normal, and we think that will continue for at least the next the next couple of years. We’ve been pricing our product with that view.”
Palo Alto’s [County, Iowa] 2022 tally of 842 farms generates nearly $800 million in annual market value. But nearly 400 small farms have been absorbed into bigger operations or otherwise stopped operating over recent decades, and Palo Alto’s population has dropped by 4,200 people since 1970.
Today’s Iowa farms are largely focused on raising hogs and growing corn, both of which are linked to numerous environmental problems. Farmers growing corn, for example, often rely heavily on applications of toxic pesticides and fertilizers, while livestock operations generate millions of tons of manure annually. The chemicals and manure pollute food and water consumed by people even far from farm fields.
When nitrogen from fertilizer and manure combine with oxygen they create nitrates, which routinely drain from farm fields into groundwater, streams, and rivers, contaminating water sources. Babies can suffer severe health problems when consuming nitrates in drinking water, and a growing body of literature indicates potential associations that include an increased risk of cancer. Exposure to elevated levels of nitrates in drinking water has been linked by researchers to cancers of the blood, brain, breast, bladder and ovaries.
As well, there are years of research showing that many herbicides and other pesticides applied to farm fields are linked to cancers and other diseases. The National Cancer Institute and the National Institute of Environmental Health Sciences have been funding research to investigate the links between disease and farming for more than 30 years, focusing their work on people in Iowa and North Carolina. Among the findings are links between pesticides and malignant brain tumors, multiple myeloma, pancreatic cancer and certain breast cancers.
Concerns about connections between the farm pollutants and cancer have been mounting, particularly in Palo Alto County, which had the highest incidence of cancer of any county in the state and the second-highest incidence of cancer among all US counties, with 83 new cases of cancer on average each year, in a population of 8,996, according to a 2023 report by US News.
Importance Many medical journals, including JAMA, restrict the use of causal language to the reporting of randomized clinical trials. Although well-conducted randomized clinical trials remain the preferred approach for answering causal questions, methods for observational studies have advanced such that causal interpretations of the results of well-conducted observational studies may be possible when strong assumptions hold. Furthermore, observational studies may be the only practical source of information for answering some questions about the causal effects of medical or policy interventions, can support the study of interventions in populations and settings that reflect practice, and can help identify interventions for further experimental investigation. Identifying opportunities for the appropriate use of causal language when describing observational studies is important for communication in medical journals.
Observations A structured approach to whether and how causal language may be used when describing observational studies would enhance the communication of research goals, support the assessment of assumptions and design and analytic choices, and allow for more clear and accurate interpretation of results. Building on the extensive literature on causal inference across diverse disciplines, we suggest a framework for observational studies that aim to provide evidence about the causal effects of interventions based on 6 core questions: what is the causal question; what quantity would, if known, answer the causal question; what is the study design; what causal assumptions are being made; how can the observed data be used to answer the causal question in principle and in practice; and is a causal interpretation of the analyses tenable?
Conclusions and Relevance Adoption of the proposed framework to identify when causal interpretation is appropriate in observational studies promises to facilitate better communication between authors, reviewers, editors, and readers. Practical implementation will require cooperation between editors, authors, and reviewers to operationalize the framework and evaluate its effect on the reporting of empirical research.
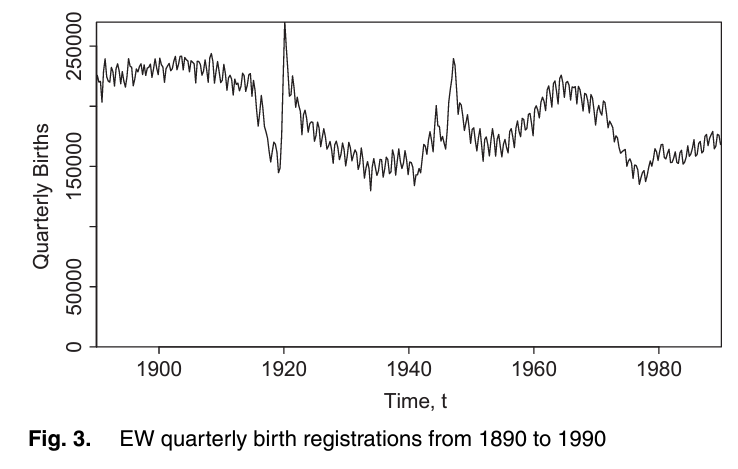
The analysis of national mortality trends is critically dependent on the quality of the population, exposures and deaths data that underpin death rates. We develop a framework that allows us to assess data reliability and to identify anomalies, illustrated, by way of example, using England and Wales population data. First, we propose a set of graphical diagnostics that help to pinpoint anomalies. Second, we develop a simple Bayesian model that allows us to quantify objectively the size of any anomalies. Two-dimensional graphical diagnostics and modelling techniques are shown to improve significantly our ability to identify and quantify anomalies. An important conclusion is that significant anomalies in population data can often be linked to uneven patterns of births of people in cohorts born in the distant past. In the case of England and Wales, errors of more than 9% in the estimated size of some birth cohorts can be attributed to an uneven pattern of births. We propose methods that can use births data to improve estimates of the underlying population exposures. Finally, we consider the effect of anomalies on mortality forecasts and annuity values, and we find significant effects for some cohorts. Our methodology has general applicability to other sources of population data, such as the Human Mortality Database.
Keywords: Baby boom;Cohort–births–deaths exposures methodology; Convexity adjustment ratio; Deaths; Graphical diagnostics; Population data
Author(s): Andrew J.G.Cairns, Heriot-Watt University, Edinburgh, UK David Blake, Cass Business School, London, UK Kevin Dowd Durham University Business School, UK and Amy R. Kessler Prudential Retirement, Newark, USA
Publication Date: 2016
Publication Site: Journal of the Royal Statistical Society
J. R. Statist. Soc. A (2016) 179, Part 4, pp. 975–1005
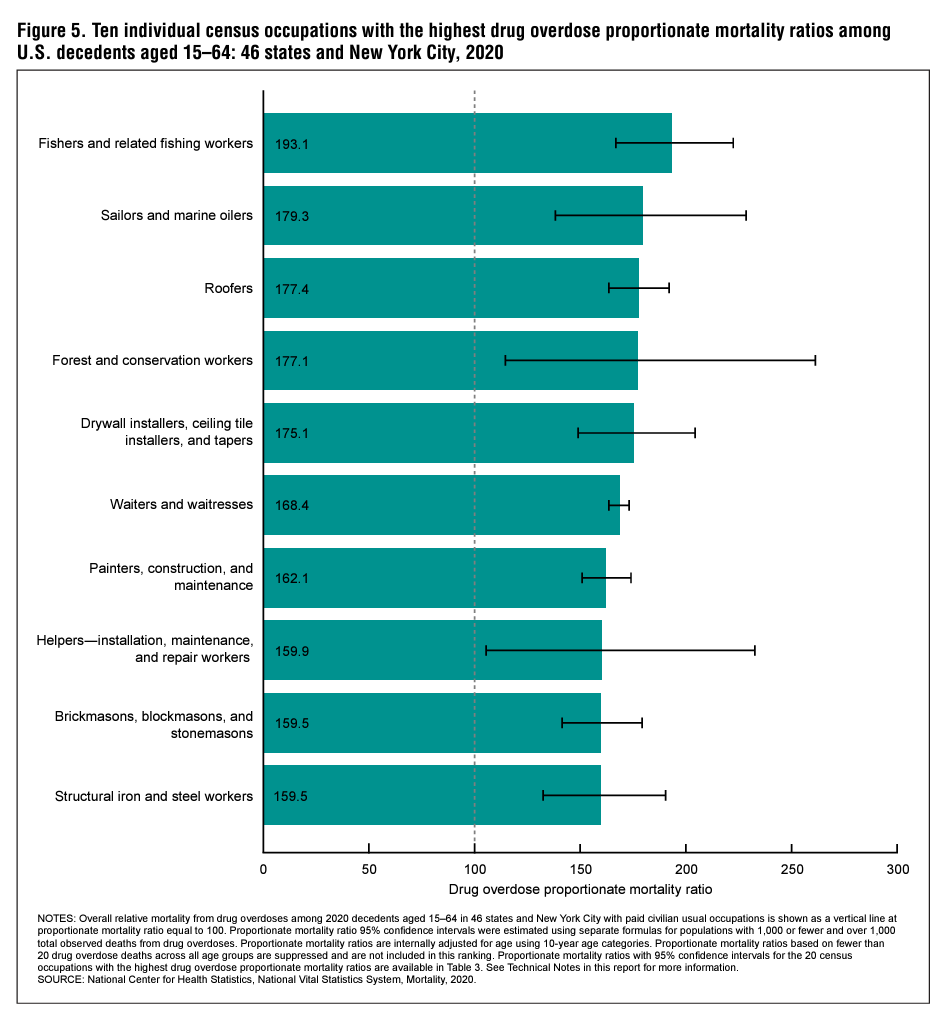
Objective—This report describes deaths from drug overdoses in 2020 in U.S. residents in 46 states and New York City by usual occupation and industry. August 22, 2023
Conclusions—Variation in drug overdose death rates and PMRs by usual occupation and industry in 2020 demonstrates the disproportionate burden of the ongoing drug overdose crisis on certain sectors of the U.S. workforce.
Methods—Frequencies, death rates, and proportionate mortality ratios (PMRs) are presented using the 2020 National Vital Statistics System mortality data file. Data were restricted to decedents aged 16–64 for rates and 15–64 for PMRs with usual occupations and industries in the paid civilian workforce. Age-standardized drug overdose death rates were estimated for usual occupation and industry groups overall, and age-adjusted drug overdose PMRs were estimated for each usual occupation and industry group overall and by sex, race and Hispanic-origin group, type of drug, and drug overdose intent. Age-adjusted drug overdose PMRs were also estimated for individual occupations and industries.
Results—Drug overdose mortality varied by usual occupation and industry. Workers in the construction and extraction occupation group (162.6 deaths per 100,000 workers, 95% confidence interval: 155.8–169.4) and construction industry group (130.9, 126.0–135.8) had the highest drug overdose death rates. The highest group-level drug overdose PMRs were observed in decedents in the construction and extraction occupation group and the construction industry group (145.4, 143.6–147.1 and 144.9, 143.2–146.5, respectively). Differences in drug overdose PMRs by usual occupation and industry group were observed within each sex, within each race and Hispanicorigin group, by drug type, and by drug overdose intent. Among individual occupations and industries, the highest drug overdose PMRs were observed in decedents who worked as fishers and related fishing occupations and in fishing, hunting, and trapping industries (193.1, 166.8–222.4 and 186.5, 161.7–214.1, respectively).
Author(s): Billock RM, Steege AL, Miniño A.
Publication Date: August 22, 2023
Publication Site: CDC, National Vital Statistics System
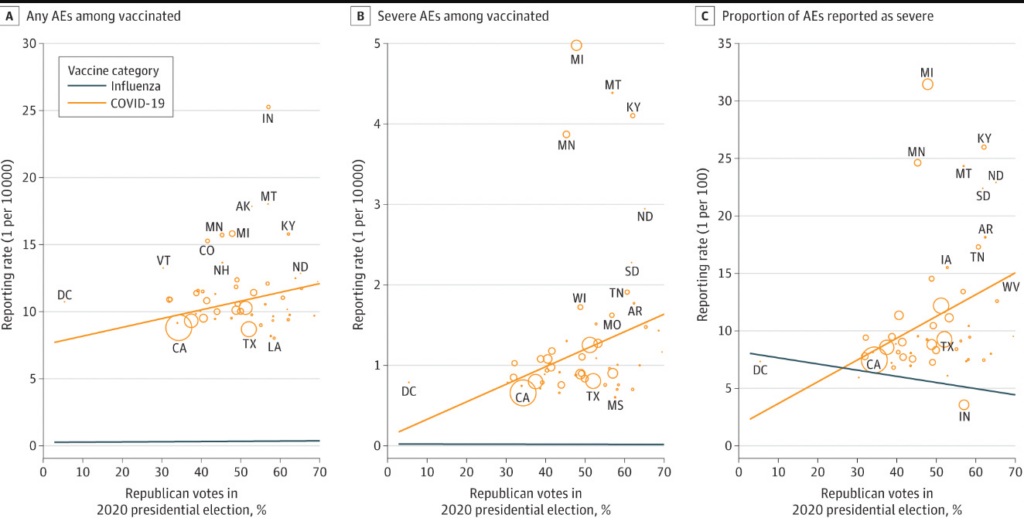
Now let’s turn to the paper. Here is what the authors find (weak correlation btw voting and vaccine injuries) , and here are the issues.
These data are ecological. It doesn’t prove that republicans themselves are more likely to report vaccine injuries. It would not be difficult to pair voting records with vaccine records at an individual patient level if the authors wished to do it right— another example of research laziness.
What if republicans actually DO have more vaccine injuries? The authors try to correct for the fact by adjusting for influenza adverse events.
Let me explain why this is a poor choice. The factors that predict whether someone has an adverse event to influenza vaccine may not be the same as those that predict adverse events from covid shots. It could be that there are actually more covid vaccine injuries in one group than another— even though both had equal rates of influenza injuries.
Another way to think of it is, there can be two groups of people and you can balance them by the rate with which they get headaches from drinking wine, but one group can be more likely to get headaches from reading without glasses because more people in that group wear glasses. In other words, states with more republicans might be states with specific co-morbidities that predict COVID vaccine adverse side effects but not influenza vaccine side effects. We already know that COVID vaccine injuries do affect different groups (young men, for e.g.).
Author(s): Vinay Prasad
Publication Date: 2 Apr 2024
Publication Site: Vinay Prasad’s Thoughts and Observations at substack
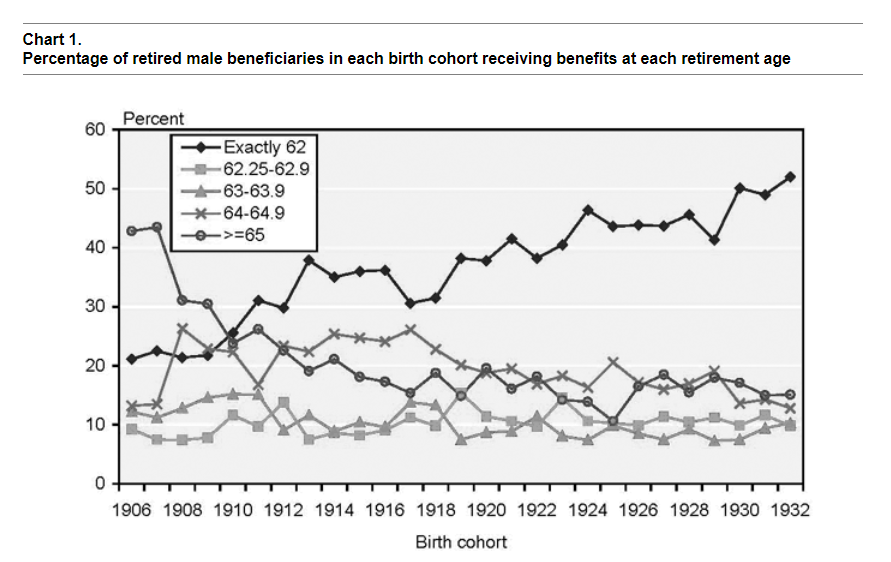
In this paper I use the 1973 cross-sectional Current Population Survey (CPS) matched to longitudinal Social Security administrative data (through 1998) to examine the relationship between retirement age and mortality for men who have lived to at least age 65 by year 1997 or earlier.1 Logistic regression results indicate that controlling for current age, year of birth, education, marital status in 1973, and race, men who retire early die sooner than men who retire at age 65 or older. A positive correlation between age of retirement and life expectancy may suggest that retirement age is correlated with health in the 1973 CPS; however, the 1973 CPS data do not provide the ability to test that hypothesis directly.
Regression results also indicate that the composition of the early retirement variable matters. I represent early retirees by four dummy variables representing age of entitlement to Social Security benefits—exactly age 62 to less than 62 years and 3 months (referred to as exactly age 62 in this paper), age 62 and 3 months to 62 and 11 months, age 63, and age 64. The reference variable is men taking benefits at age 65 or older. I find that men taking benefits at exactly age 62 have higher mortality risk than men taking benefits in any of the other four age groups. I also find that men taking benefits at age 62 and 3 months to 62 and 11 months, age 63, and age 64 have higher mortality risk than men taking benefits at age 65 or older. Estimates of mortality risk for “early” retirees are lowered when higher-risk age 62 retirees are combined with age 63 and age 64 retirees and when age 62 retirees are compared with a reference variable of age 63 and older retirees. Econometric models may benefit by classifying early retirees by single year of retirement age—or at least separating age 62 retirees from age 63 and age 64 retirees and age 63 and age 64 retirees from age 65 and older retirees—if single-year breakdowns are not possible.
The differential mortality literature clearly indicates that mortality risk is higher for low-educated males relative to high-educated males. If low-educated males tend to retire early in relatively greater numbers than high-educated males, higher mortality risk for such individuals due to low educational attainment would be added to the higher mortality risk I find for early retirees relative to that for normal retirees. Descriptive statistics for the 1973 CPS show that a greater proportion of age 65 retirees are college educated than age 62 retirees. In addition, a greater proportion of age 64 retirees are college educated than age 62 retirees, and a lesser proportion of age 64 retirees are college educated than age 65 or older retirees. Age 63 retirees are only slightly more educated than age 62 retirees.
Despite a trend toward early retirement over the birth cohorts in the 1973 CPS, I do not find a change in retirement age differentials over time. However, I do find a change in mortality risk by education over time. Such a change may result from the changing proportion of individuals in each education category over time, a trend toward increasing mortality differentials by socioeconomic status, or a combination of the two.
This paper does not directly explore why a positive correlation between retirement age and survival probability exists. One possibility is that men who retire early are relatively less healthy than men who retire later and that these poorer health characteristics lead to earlier deaths. One can interpret this hypothesis with a “quasidisability” explanation and a benefit optimization explanation. Links between these interpretations and my analysis of the 1973 CPS are fairly speculative because I do not have the appropriate variables needed to test these interpretations.
A quasi-disability explanation, following Kingson (1982), Packard (1985), and Leonesio, Vaughan, and Wixon (2000), could be that a subgroup of workers who choose to take retired-worker benefits at age 62 is significantly less healthy than other workers but unable to qualify for disabled-worker benefits. An econometric model with a mix of both these borderline individuals and healthy individuals retiring at age 62 and with almost no borderline individuals retiring at age 65 could lead to a positive correlation between retirement and mortality, even if a greater percentage of individuals who retire at age 62 are healthy than unhealthy. Evidence for this hypothesis can be inferred from the finding that retiring at exactly age 62 increases the odds of dying in a unit age interval by 12 percent relative to men retiring at 62 and 3 months to 62 and 11 months for men in the 1973 CPS. In addition, retiring exactly at age 62 increases the odds of dying by 23 percent relative to men retiring at age 63 and by 24 percent relative to men retiring at age 64. A group with relatively severe health problems waiting for their 62nd birthday to take benefits could create this result.
An explanation based on benefit optimization follows Hurd and McGarry’s research (1995, 1997) in which they find that individuals’ subjective survival probabilities roughly predict actual survival. If men in the 1973 CPS choose age of benefit receipt based on expectations of their own life expectancy, then perhaps a positive correlation between age of retirement and life expectancy implies that their expectations are correct on average. If actuarial reductions for retirement before the normal retirement age are linked to average life expectancy and an individual’s life expectancy is below average, it may be rational for that individual to retire before the normal retirement age. Evidence for this hypothesis can be inferred from the fact that men retiring at age 62 and 3 months to age 62 and 11 months, age 63, and age 64 all experience greater mortality risk than men retiring at age 65 or older. If only men with severe health problems who are unable to qualify for disability benefits are driving the results, we probably would not expect to see this result. We might expect most of these individuals to retire at the earliest opportunity (exactly age 62).2
Author(s): Hilary Waldron
Publication Date: August 2001
Publication Site: Social Security Office of Policy, ORES Working Paper No 93
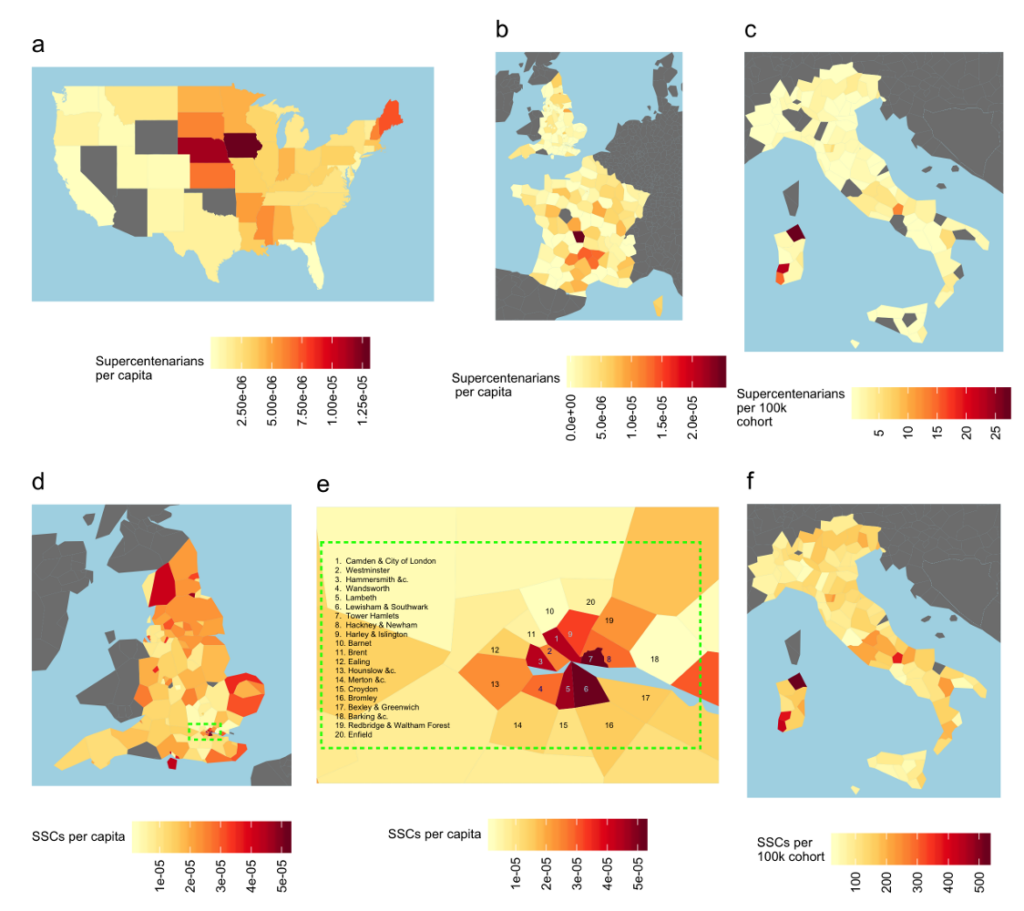
The observation of individuals attaining remarkable ages, and their concentration into geographic sub-regions or ‘blue zones’, has generated considerable scientific interest. Proposed drivers of remarkable longevity include high vegetable intake, strong social connections, and genetic markers. Here, we reveal new predictors of remarkable longevity and ‘supercentenarian’ status. In the United States, supercentenarian status is predicted by the absence of vital registration. The state-specific introduction of birth certificates is associated with a 69-82% fall in the number of supercentenarian records. In Italy, England, and France, which have more uniform vital registration, remarkable longevity is instead predicted by poverty, low per capita incomes, shorter life expectancy, higher crime rates, worse health, higher deprivation, fewer 90+ year olds, and residence in remote, overseas, and colonial territories. In England and France, higher old-age poverty rates alone predict more than half of the regional variation in attaining a remarkable age. Only 18% of ‘exhaustively’ validated supercentenarians have a birth certificate, falling to zero percent in the USA, and supercentenarian birthdates are concentrated on days divisible by five: a pattern indicative of widespread fraud and error. Finally, the designated ‘blue zones’ of Sardinia, Okinawa, and Ikaria corresponded to regions with low incomes, low literacy, high crime rate and short life expectancy relative to their national average. As such, relative poverty and short lifespan constitute unexpected predictors of centenarian and supercentenarian status and support a primary role of fraud and error in generating remarkable human age records.
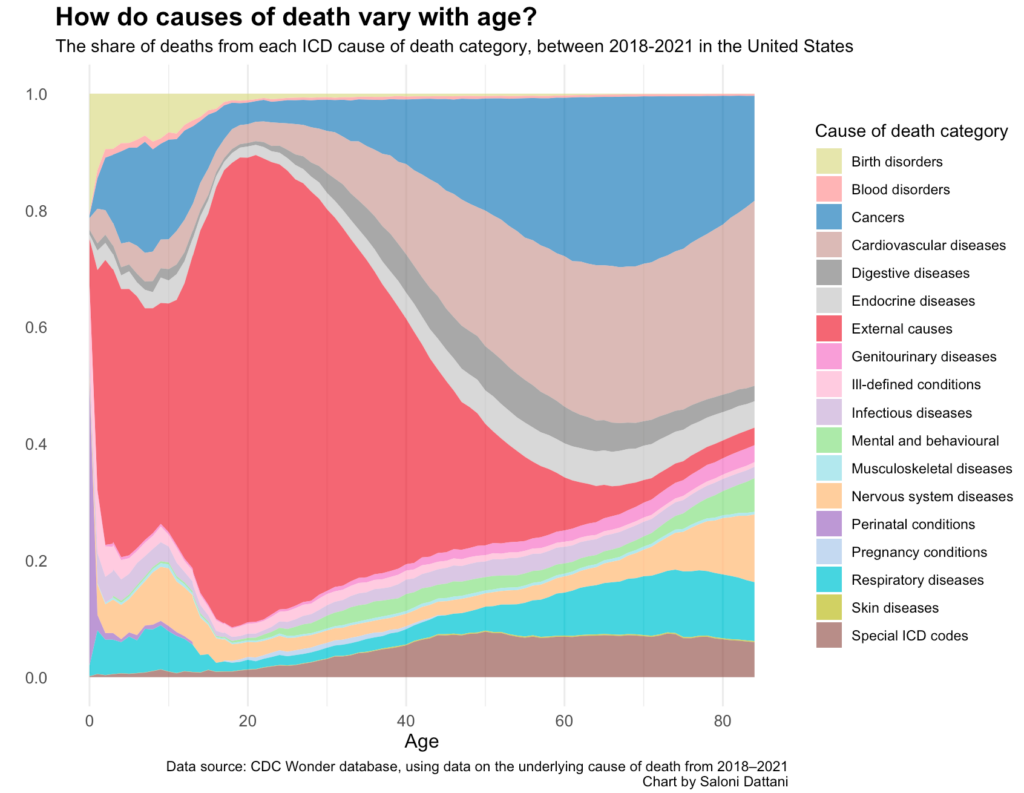
You can see that, in childhood, in the US, the most common causes of death are ‘external causes’. This is a broad category that includes accidents, falls, violence, and overdoses, and is shown in red. But there’s also a notable contribution from birth disorders (in muted green), childhood cancers (in blue), and respiratory diseases (in cyan).
The share of deaths in childhood from cancers stood out to me. We’ve seen lots of progress against many childhood cancers over the last 50 years — notably in treating leukemia, brain cancers, kidney cancers, lymphomas, and retinoblastoma — but this is a reminder that there’s still further to go.
From adolescence until middle-age, ‘external causes’ are now the overwhelming cause of death. Around 80% of deaths at the age of 20 in the US are due to external causes. These result from causes such as accidents, violence, and overdoses.
At older ages, diseases rise in importance. Causes of death also become more varied, although cardiovascular diseases and cancers are the most common.
You might also be wondering about the brown category at the bottom, called ‘special ICD codes’. That’s a placeholder category in the system for deaths caused by new diseases — predominantly Covid-19, since the data spans 2018 to 2021.3